
Preparing Physically for Birth
Pelvic Floor Exercises
Somewhere in your 3rd trimester (if not sooner), you should include in your weekly workouts certain poses that can strengthen, lengthen and relax your pelvic floor. This will also help with incontinence and postpartum recovery.
We don’t want our pelvic floors to be tight/gripped or loose - we want them strong and flexible, so we can engage them when needed and release when needed.
Squats
Holding a deep squat (i.e. Malasana in yoga)
Parallel squats: keep your toes pointing forward, go down until your thighs are parallel to floor
Sumo squats: feet wider and toes pointing slightly outward
Wall Squats: keep your back against the wall to maintain good posture while you hold squat for 30 secs or so
Pelvic Tilts
Cat pose: round your back up, tilting your pelvis down
Instead of countering this motion with Cow pose, return just to Table pose - cow can put too much pressure on your spine and overstretch your ab muscles
Bridge pose: slowly lift and lower your hips while lying on your back, to open up hips and relieve pressure
Child’s pose or puppy’s pose (similar but hips go up to the ceiling, kind of a cross between child’s and downward dog)
This post highlights a few other movements that can prepare your pelvic floor; also consider following Vagina Whisperer (prenatal & postpartum)
Kegel contractions
Kegels can be pretty boring to do on their own, so instead see if you can incorporate them into other exercises - for instance, every time you raise up for a bridge pose or round into a cat pose, add a Kegel
In addition to the squeezing in of the traditional Kegel, pair this with a “reverse Kegel” where you fully release any engagement. This combo of activation and release is exactly what you’ll need to give birth.
“Mindful pooping”
Prepare for the pushing stage of labor by bringing more awareness to the muscles you use when you’re pooping, as this is similar to what you’ll engage for pushing
Especially important if planning to have an epidural, since you will rely more on muscle memory for pushing, rather than sensory feedback
Perineal Stretching
The reality is that much of your experience with regards to labor length/pain, vaginal tearing and injury is out of your control
That said, there is some evidence that perineum stretching can help first time mothers avoid serious tearing or needing an episiotomy (when they have to cut the area between your vagina and anus to make more room for baby - this is quite uncommon, only around 5% at CPMC Van Ness).
In the last month before your due date, consider doing perineum stretching 1-2x per week for about 10 minutes at a time
Wash your hands and lubricate your thumbs with a cooking oil (olive, vegetable, almond) or KY Jelly, or your body’s own vaginal lubricant. Don’t use baby oil or petroleum jelly.
Insert your thumbs about 1-1.5 inches into the the vagina (about to the knuckle)
Press down on the perineum towards your anus until you feel a slight burning or stretching feeling (uncomfortable, but not painful). Hold this for 1-2 minutes
Then, bring your thumbs upwards and outwards into a U shape (i.e. up from 6 o’clock to 9 and 3 o’clock), stretching and massaging back and forth slowly
This is a good opportunity to practice slow, deep breathing and muscle relaxation


Finally, as part of your “birth preferences”, I highly recommend you request that the nurses provide warm compresses to your perineum during pushing/delivery; this can also prevent tearing
If you’re based in SF and interested in going deeper on this topic, Britt Forhman is awesome and teaches a class at Natural Resources “Preparing your Vagina for Birth”
Learn (but don’t freak about) your baby’s positioning
Your baby will change positions a ton during pregnancy, so don’t worry about the positioning until the very end (last week or so)
Your OB should be able to tell you how the baby is positioned just by feeling, but may want to confirm a sub-optimal position via ultrasound. Below are the main 4 positions:
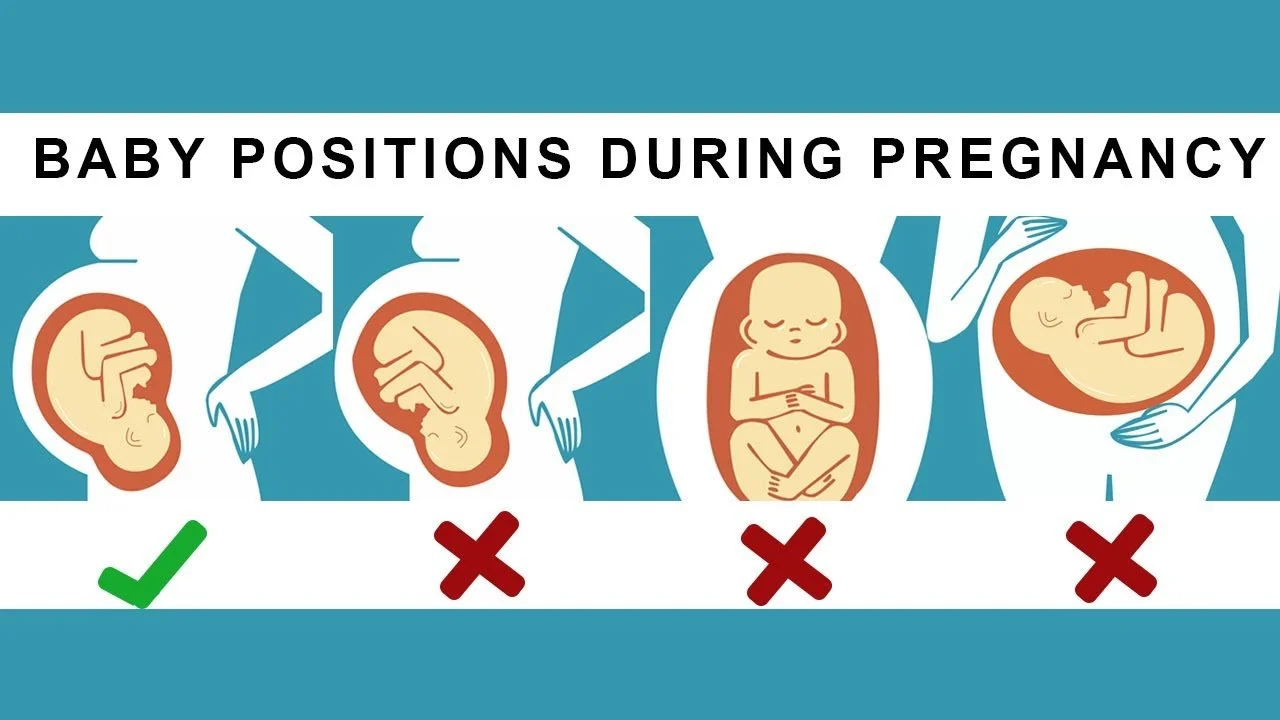
Anterior: this is the optimal position for birth, and the most common. Baby is head down and their face is facing your back; their back is towards the front of your stomach. The smallest part of the baby’s head leads the way through the cervix which helps open it up naturally and less painfully.
Posterior (“sunny-side up”) is the opposite: the baby is also head down, but they are facing your stomach, so you are back-to-back. The majority of posterior babies end up rotating into anterior on their own, but if they remain in posterior it can lead to lots of back pain during labor and longer deliveries.
Breech is when baby is feet or butt first, which can make it much harder to get through the birth canal and increases risk of umbilical cord wrapping issues. In about 50% of cases, your doctor may be able to help turn the baby around. Otherwise, a C-section may be necessary.
Transverse is when baby is lying sideways in the uterus. Most babies get out of this position by their due date, but if not a C-section may be necessary.
Many people believe that certain exercises and movements can use gravity to encourage the baby to get into the anterior position. These include:
Getting into the hands-and-knees position for at least 10 minutes daily
Walking regularly
Sitting with your pelvis tilted forward rather than backward
Inversions: any position where your chest is lower than your hips (e.g. your legs are up on the couch and you’re leaning forward with your arms on the ground)
Many other exercises promoted by the organization Spinning Babies
While these are all healthy exercises to do anyway, the research on this topic suggests it doesn’t actually make a difference. Chances are your baby will move into the right position on its own; and if it doesn’t, your doctor may be able to coax it into position through ECV (external cephalic version), basically applying pressure from the outside.